Shoulder Special Tests
Special tests are techniques utilized by clinicians to test the structural integrity of tissues within the body. All tests must be done bilaterally to determine if results are abnormal. Each individual will display unique results of each test based on their anatomical make up.
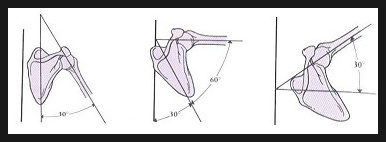
Scapulothoracic Rhythm
0-30 degrees= Abduction occurs primarly at the glenohumoral joint.
30-90 degrees= Abduction occurs at a 1:1 ratio between the glenohumoral joint and scapulothoracic joint
90- End of ROM= Abduction occurs at a 2:1 ratio with the scapulothoracic joint moving twice as much as the glenohumoral joint.
30-90 degrees= Abduction occurs at a 1:1 ratio between the glenohumoral joint and scapulothoracic joint
90- End of ROM= Abduction occurs at a 2:1 ratio with the scapulothoracic joint moving twice as much as the glenohumoral joint.
http://www.geocities.ws/ptexas9/movements.html (retrieved 10/20/2013)
YergasonsPatient/ Examiner Position:: Hook Seated
Elbow Flexed at 90 degrees Procedure: The examiner provides resistance while the patient concurrently moves the GH joint into external rotation and supination. The examiner palpates the bicipital groove. PositiveTest: Sprain to the transverse ligament. Anterior/ Posterior DrawerPatient/ Examiner Position: Hook seated or supine, shoulder abducted to 90 degrees, and elbow flexed to 90 degrees. Examiner stands next to the involved shoulder placing one hand anround the humerus. The other hand stabilizes the scapula, fingers over scapula, thumb over coracoid process.
Procedure: The subject must remain relaxed while examiner firmly glides the head of the humerus anteriorly and posteriorly while applying slight distraction to the glenohumeral joint. Positive Test: Increased anterior/ posterior translation of the humeral head. ClunkPatient/ Examiner Position: The subject lies supine of the table. The examiner places one hand on the posterior aspect of the subject's humeral head and the the other hand on the distal humerus.
Procedure: The examiner passively abducts and externally rotates the subject's arm over head and applies an anterior force to the humerus at the same time the examiner circumducts the humeral head around the glenoid labrum. Positive Test: Grinding or clunking sensation may be indicative of a glenoid labrum tear. ApprehensionPatient/ Examiner Position: The subject lies supine of the table.
Procedure: With the subjects involved shoulder in 90 degrees of abduction and the elbow in 90 degrees of flexion, the examiner slowly externally rotates the shoulder. Positive Test: Subject looks apprehensive or expresses feelings of apprehension toward further movement in the externally rotated direction. Positive test may be indicative of a past shoulder dislocation. Special Considerations: Simple indication or reporting of apprehension to a movement does not necessarily indicate a dislocation of the glenohumeral joint Jobe RelocationPatient/ Examiner Position: the subject lies prone with the test shoulder in 90 degrees of abduction and full external rotation. The examiner stands with the distal hand grasping the subject’s wrist and hand. The examiner’s proximal hand is placed over the subject’s humeral head
Procedure: the examiner applies a posterior force to the humeral head while the examiner externally rotates the subject's humerus. Positive Test: a reduction of pain and apprehension, and commonly an increase in shoulder external rotation, are indicative of anterior instability Special Considerations: This test should be performed immediately following the apprehension test. Pain associated with the Jobe relocation test that follows a positive anterior apprehension test may be associated with any number of pathologies not limited to anterior instability. However, if pain is seen with an anterior apprehension test and subsides with a subsequent Jobe relocation test, it is quite possible that any pain was in fact associated with a greater than normal anterior gliding of the humeral head SulcusPatient/ Examiner Position: the subject sits with the forearms and hands resting in the lap. The examiner stands with the proximal hand grasping the subject’s scapula (superiorly) and the distal hand grasping the subject’s elbow
Procedure: with the scapula stabilized, the examiner applies an inferior (distraction) force with the distal hand. Positive Test: excessive inferior humeral head translation with a visible and/or palpable “step-off” or “sulcus” deformity immediately inferior to the acromion (laterally) is indicative of inferior and/or multidirectional instability Acromioclavicular ShearPatient/ Examiner Position: The subject sits with the involved arm relaxed at the side. The examiner stands on the involved side, placing one hand on the subject’s clavicle and the other hand on the spine of the scapula.
Procedure: The examiner gently squeezes the hands together, noting any movement at the acromioclavicular joint Positive Test: Pain and/or movement of the clavicle is a positive indication of an acromioclavicular and/or coracoclavicular ligament sprain. Special Considerations: this test should not be performed if there is obvious acromioclavicular joint deformity Pectoralis Major ContracturePatient/ Examiner Position: The subject lies supine with both hands clasped together behind the head. The examiner stands directly behind the subject.
Procedure: The examiner passively moves the subject’s elbows toward the table. The subject is asked to relax the upper extremity musculature during this movement. Positive Test: A pectoralis major muscle contracture is suspected if the subject is unable to passively have his elbow (s) reach the table. Special Considerations: It is important to be sure the subject is relaxed and no upper trunk rotation occurs, allowing for one side to appear restricted. This test is primarily used to assess tissue extensibility and should not be accompanied by any unexplained shoulder pain. Drop ArmPatient/ Examiner Position: The subject sits on a table or stands.
Procedure: The examiner passively abducts the subject’s involved arm to 90 degrees and then instructs the subject to slowly lower the arm to the side. Positive Test: The subject is unable to slowly return the arm to the side and/or has significant pain when attempting to perform the task. This is indicative of rotator cuff pathology. Special Considerations: if the examiner suspects rotator cuff pathology prior to performing the test, he should prepare to rapidly assist the subject in the event that the subject does experience an inability to control the adduction movement of the arm. Empty CanPatient/ Examiner Position: The subject stands with both shoulders abducted to 90 degrees, horizontally adducted 30 degrees, and internally rotated so the subject’s thumbs face the floor.
Procedure: The examiner resists the subject’s attempts to actively abduct both shoulders Positive Test: Involvement of the supraspinatus muscle and/or tendon is suspected with noted weakness and/or a report of pain Special Considerations: Weakness of the supraspinatus muscle may be a result of suprascapular nerve involvement. Reported pain may be indicative of tendinitis and/or impingement Cross over ImpingmentPatient/ Examiner Position: The subject sits. The examiner stands with one hand on the posterior aspect of the subject’s shoulder to stabilize the trunk and the other hand grasping the subject’s elbow on the test arm.
Procedure: With the subject’s trunk stabilized, the examiner passively and maximally adducts the test shoulder Positive Test: Superior shoulder pain is indicative of acromioclavicular joint pathology. Anterior shoulder pain is indicative of subscapularis, supraspinatus, and/or biceps long head pathology. Posterior shoulder pain is indicative of infraspinatus, teres minor, and/or posterior capsule pathology Hawkins- Kennedy Impingment Patient/ Examiner Position: The subject sits or stands with both upper extremities relaxed. The examiner stands with one hand grasping the subject’s elbow and the other hand grasping the subject’s wrist, both on the test arm.
Procedure: The examiner forward flexes the shoulder to 90 degrees and then internally rotates the subject’s test shoulder Positive Test: Shoulder pain and apprehension are indicative of shoulder impingement, particularly of the supraspinatus tendon Special Considerations: This test tends to be the most sensitive for assessing subacromial impingement. Supine ImpingmentPatient/ Examiner Position: Patient is in a supine position with examiner at the side of the involved arm.
Procedure: Examiner grasps the patient’s wrist and distal aspect of the humerus and abducts the patient’s arm,with a fully etended elbow, to end range. Examiner moves the patient’s arm into external rotation and adducts the arm to the patient’s ear. Next, the examiner internally rotates the arm. Positive Test: A positive test is indicated by significant increase in shoulder pain Military Brace PositionPatient/ Examiner Position: The subject stands in the anatomical position
Procedure: The examiner stands behind the subject and unilaterally assesses the radial pulse. The subject’s same arm is then passively extended and abducted to 30 degrees by the examiner, while the subject simultaneously hyperextends the head and neck. Positive Test: A diminished or absent radial pulse may indicate potential thoracic outlet syndrome. Special Considerations: The subject should assess rate and rhythm of the pulse and note any changes. This assessment should be compared bilaterally. This test is also called the costoclavicular syndrome test, as it is believed a positive finding may be related to a compression of the subclavian artery as it travels under the clavicle and ribs. Adson's ManeuverPatient/ Examiner Position: The subject sits or stands. The examiner stands with fingers over the radial artery (distally).
Procedure: The examiner externally rotates and extends the subject’s test arm while palpating the radial while palpating the radial pulse. The subject then extends and rotates the neck toward the test arm and takes a deep breath. Positive Test: A diminished or absent radial pulse is indicative of thoracic outlet syndrome, secondary to compression of the subclavian artery by the scalene muscles. Special Considerations: This test assesses vascular structures only and has a high incidence (>50%) of false positive findings. The examiner should record the rate and rhythm of the pulse as reduced or altered, as opposed to one that is completely diminished. Allen'sPatient/ Examiner Position: The subject sits or stands with the test shoulder in 90 degrees of abduction and external rotation, and the elbow in 90 degrees of flexion. The examiner stands with fingers over the radial artery.
Procedure: The subject rotates the neck away from the test arm while the examiner palpates the radial pulse. Positive Test: A diminished or absent radial pulse is indicative of thoracic outlet syndrome. Special Considerations: This test assesses vascular structures only and has a high incidence (>50%) of false positive findings. The examiner should record the rate and rhythm of the pulse as reduced or altered, as opposed to one that is completely diminished. LudingtonsPatient/ Examiner Position: The subject sits or stands while the examiner stands directly behind the subject. The subject interlocks his fingers and places them on the superior/posterior aspect of his/her head
Procedure: The examiner palpates the long head of the biceps tendon bilaterally while the subject contracts both the left and right biceps brachii muscles simultaneously Positive Test: Increased pain is indicative of a biceps brachii long head tendinitis. Decreased tension of the tendon with palpation may indicate an inability or apprehension of the biceps brachii to contract forcefully Special Considerations: The subject should be sure to stabilize the humeral head during the contraction and allow for the hands to push into the stabilized humeral head. No tension may be the result of a biceps brachii long head rupture. SpeedsPatient/ Examiner Position: The subject sits on a table or stands. The involved shoulder is flexed to 90 degrees, the elbow is fully extended, and the forearm is supinated. The examiner places one hand along the volar aspect of the subject’s forearm and the other hand on the proximal aspect of the subject’s humerus near the area of the bicipital groove
Procedure: The examiner resists the subject’s attempt to actively flex the humerus forward Positive Test: Tenderness and/or pain in the bicipital groove is a positive finding that may suggest bicipital tendinitis Special Considerations: The examiner should carefully watch that the forearm is supinated and that the subject does not use accessory muscles to mask any existing weakness |
|
